Closing an Open Bite with Clear Aligners: Angie’s Story
A step-by-step case study on treating tongue thrust-related anterior open bite with lingual attachments, and why the right post-treatment plan is just as important as the aligners themselves
Dr. Dadjoo
Orthodontist | Porter Ranch, CA | 818-831-7600
Angie came in for what she thought was a routine retainer check. She’s a working professional in health care, someone who notices things. What she didn’t realize was that over time, a habit called tongue thrusting had quietly shifted her bite in a way that no retainer adjustment could fix on its own.
Or it’s also a clinical explainer for anyone wondering what an open bite actually is and how clear aligners can close it and what keeps it closed for good.
What Is an Anterior Open Bite?
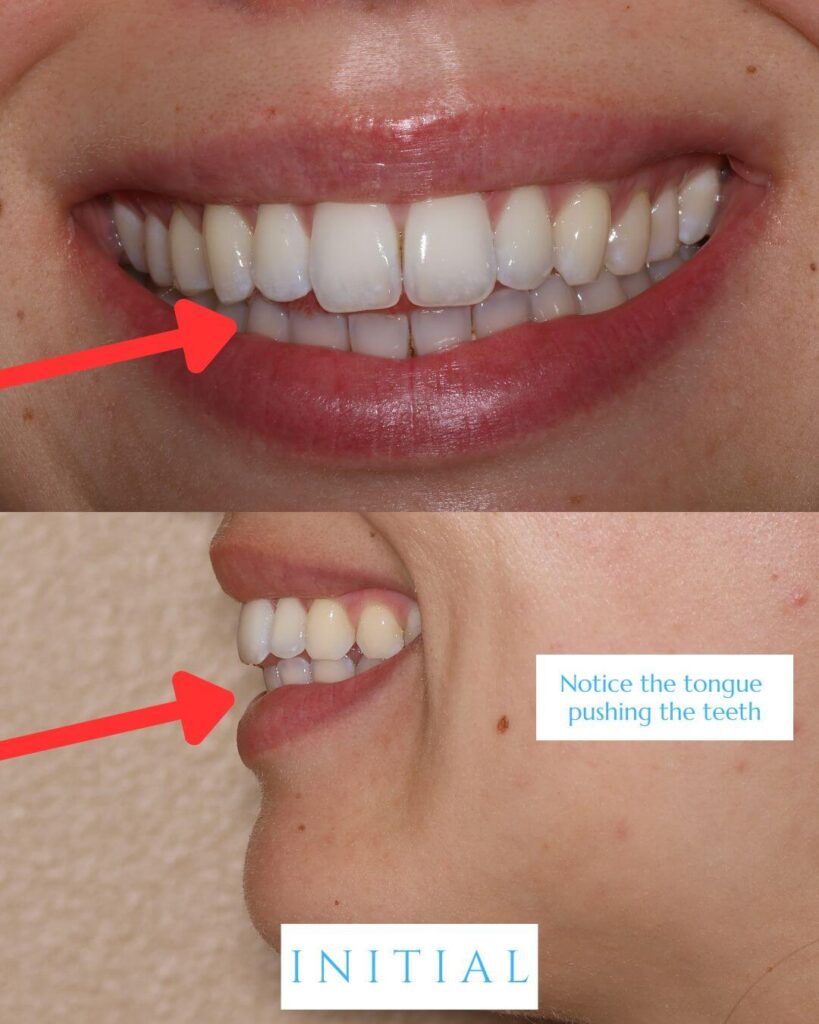
It is exactly what it sounds like. When you close your teeth together, the upper and lower front teeth don’t touch. There is a visible gap between them.
In Angie’s case, her clinical photos showed a classic pattern of tongue tip protrusion, also called tongue thrusting, where the tongue pushes forward against or between the front teeth during swallowing and at rest. This is a topic that we studied extensively during my residency at the University of Rochester Eastman Institute for Oral Health.
That constant pressure can cause the front teeth to flare outward and upward, creating two related problems:
- An anterior open bite, a gap between the upper and lower incisors
- Excessive overjet, where the space between the upper teeth protrudes significantly beyond the lower teeth
Would hold the teeth where they are, I explain to Angie, but without actually moving them back into proper alignment, the bite would remain open. That underlying habit, the tongue thrusting, would continue to work against any retainer I make over time.
Immediately, she elected to move forward with clear aligner treatment. I estimated it would take about six months and about three visits, where she comes in every 12 weeks.
What Are Attachments — and Why Do They Matter?
Clear aligners work by applying controlled pressure to the teeth. But for more complex movements — especially in the vertical dimension — aligners need a little help gripping the teeth in a precise way. That’s where attachments come in.
CLINICAL NOTE
Attachments are small, tooth-colored resin shapes that bond directly to the enamel surface of specific teeth. Think of them as clear braces: they give the aligner a mechanical anchor point to execute prescribed movements that the aligner alone couldn’t reliably accomplish. Different movements call for different attachment shapes.
For an open bite case, the primary goal is intrusion of the posterior teeth and extrusion of the anterior teeth — essentially, we want to encourage the front teeth to move down and into contact. To support extrusive movement on the upper incisors, we typically use what are called extrusion attachments.
Angie’s Specific Request: Lingual Attachments
Here’s where Angie’s case became particularly interesting from a clinical planning standpoint.
Angie works in healthcare. She’s around patients and colleagues every day. She absolutely wanted treatment — but she had one non-negotiable: she did not want visible attachments on the front surfaces of her upper front teeth (upper 2-to-2, or the six upper front teeth).
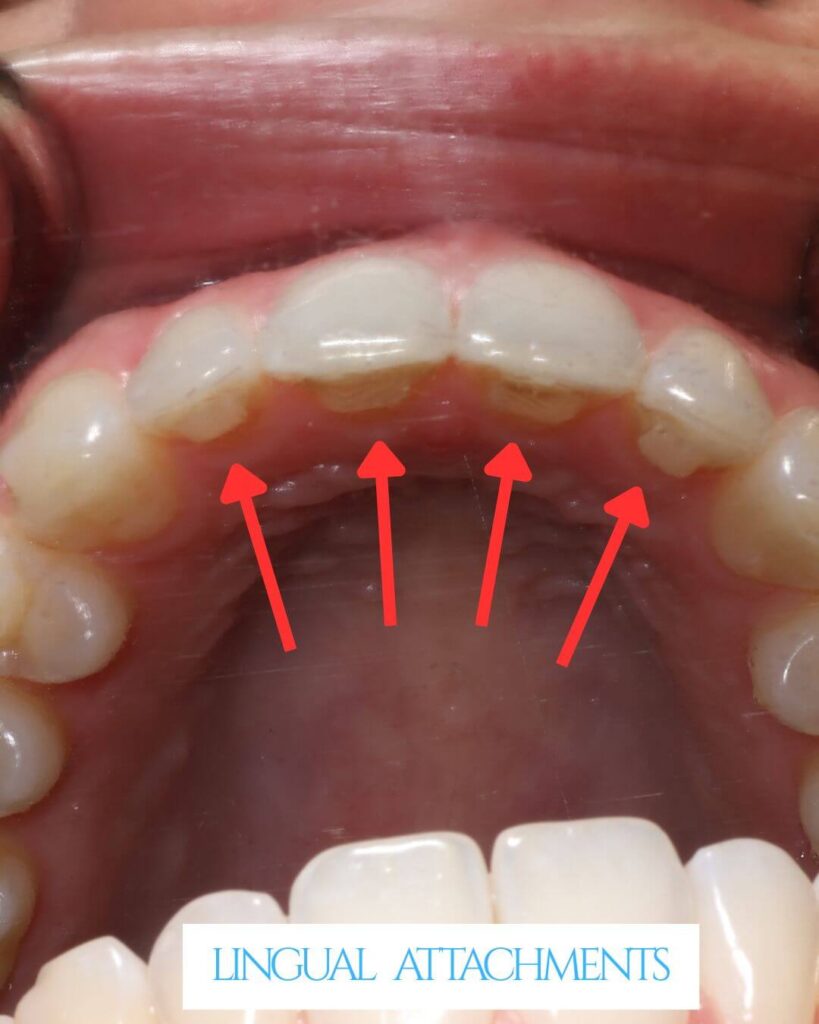
Her ask: could the attachments be placed on the back side of the teeth — the lingual surface— instead?
The answer was yes. Lingual attachment placement is more technically demanding, but it is absolutely achievable — and in Angie’s case, it was the right call. It allowed us to deliver the extrusive force needed to close the bite while keeping her smile completely attachment-free from the front.
The Treatment Journey: Three Visits, Six Months
One of the things patients always want to know is: how long will this take? Angie’s case is a great example of what focused, well-planned clear aligner treatment can accomplish in a relatively short timeframe.
Three visits. Six months. A closed bite — and a patient who could smile through every one of those months without visible hardware on her front teeth.
The Part Most People Miss: Keeping It Closed
This is the piece that separates a good orthodontic result from a lasting one.
An open bite caused by tongue thrusting will relapse if the underlying habit isn’t addressed. Aligners close the bite. Myofunctional therapy retrains the tongue.
Myofunctional therapy is a specialized form of oromuscular rehabilitation that works on tongue posture, swallowing patterns, and breathing habits. For Angie, we coordinated her aligner treatment with a referral to a myofunctional therapist — so that as her teeth moved into proper position, her tongue was simultaneously learning a new resting posture and a new swallowing pattern.
She’s doing beautifully. The results are holding. That’s the goal.

What This Case Teaches Us
A few takeaways worth highlighting — whether you’re a patient researching your own treatment options or a colleague working through a similar case:
- Open bites often have a cause beyond the teeth. Tongue position, swallowing habits, and breathing patterns all shape the bite over time. Treating the teeth without addressing the habit is treating the symptom.
- Clear aligners can close open bites — but attachment design and placement are critical. This is not a case type for guesswork.
- Patient preferences can be accommodated without compromising clinical outcomes. Lingual attachments require more planning, but the result was identical to what buccal attachments would have delivered.
- Myofunctional therapy is not optional in tongue-thrust cases. It is the retention mechanism for the bite correction.
Angie’s case is a reminder that a “simple retainer check” can be the starting point for something genuinely transformative — when a clinician is paying close attention.
Questions about your bite? Lets talk.
Dr. Dadjoo sees patients in Porter Ranch, CA. If you’re noticing a gap between your front teeth, or if you’ve been told you have a tongue thrust habit, we’d love to evaluate your case.
19950 Rinaldi Street, Suite 306, Porter Ranch, CA 91326
Expert Hands. Personal Smiles



